Open Orphan plc changes its name to hVIVO plc, learn more here.

Open Orphan plc changes its name to hVIVO plc, learn more here.
So we know, or at least it is being widely reported, that depression and anxiety indices are raised worldwide, and most especially in High Income Countries (HIC). Whilst this is a genuine concern for societies emerging from lockdown, with many now possibly mentally ill-prepared to cope with a reinvigorated social and work schedule, one of the treatments commonly used to treat depression and GAD of is raising hopes that there may be light at the end of more than one tunnel.
A recent meta-analysis of a small number of fluvoxamine efficacy trials enrolling just over 2,000 patients found that fluvoxamine reduces the chances of severe hospitalisation by up to 95%. If this efficacy is maintained in larger studies, fluvoxamine could be an important component of the Test-to-Treat strategy that the US is in the process of rolling out. Fluvoxamine was not developed as an anti-COVID drug. It has long been used as a mood-stabilizing selective serotonin reuptake inhibitor (SSRI) and is now available as an inexpensive generic drug worldwide:
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2790742
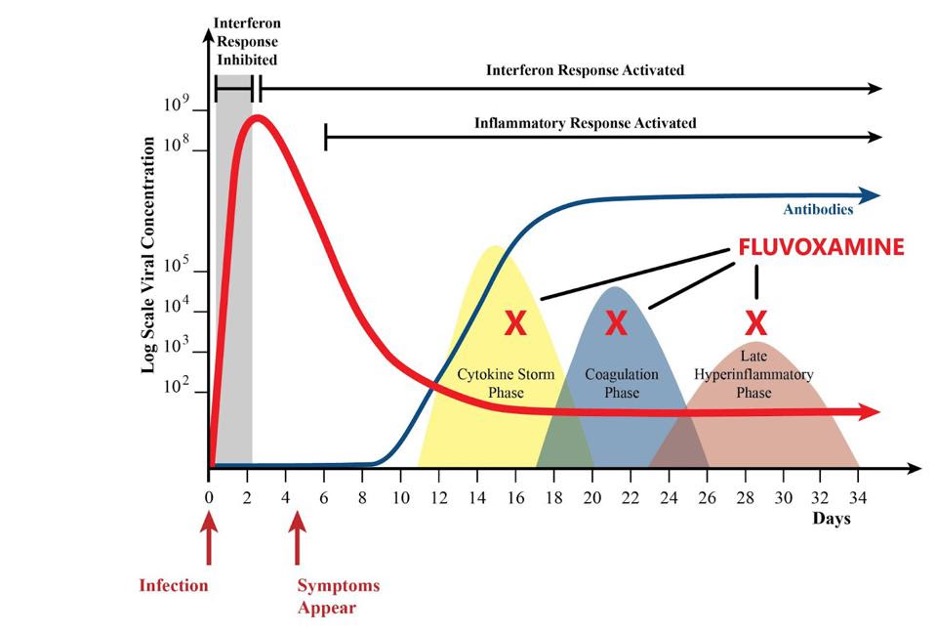
The apparent effectiveness of fluvoxamine raises the question of how it might act independently of its use as a mood stabilizer. The following provides details of the potential mechanisms by which fluvoxamine has the potential to interfere with the most severe consequences of COVID 19 infection, including cytokine storms, coagulation, and hyperinflammation.
https://pubmed.ncbi.nlm.nih.gov/33959018/
There are six known mechanisms, potentially more, by which fluvoxamine may act to treat late-stage COVID and prevent late-stage sequela: reduction In platelet aggregation, decreased mast cell degranulation, interference with endolysosomal viral trafficking and membrane binding, sigma-1 receptor activity and increased melatonin levels:
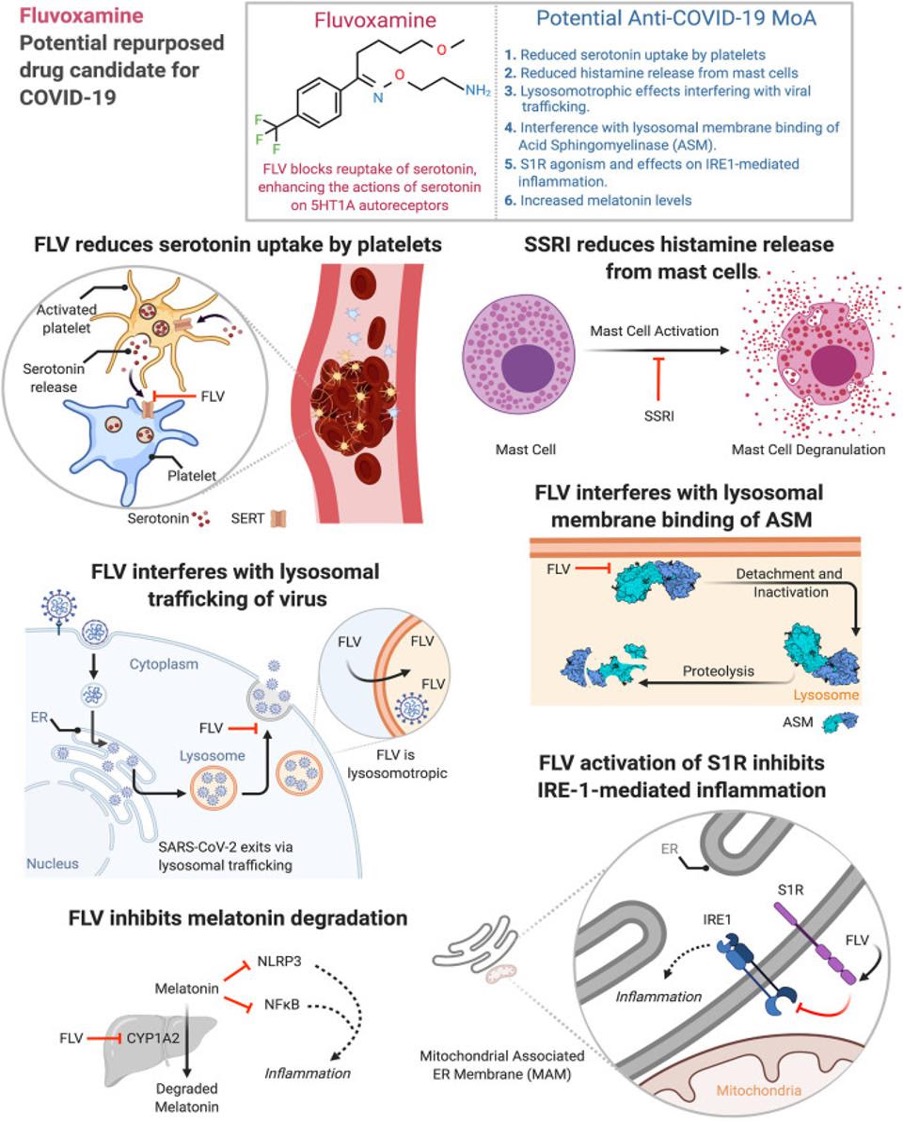
One of the primary triggers of the cytokine storm is the interaction between SARS-CoV-2 and human mast cells, which are often viral reservoirs for RNA viruses. Pulmonary tissues in the lungs of deceased COVID patients are often linked to activated mast cells, which are degranulated by viruses upon infection. Fluvoxamine also interacts with mast cells, decreasing mRNA levels of protease-1, which promotes mucosal permeability in intestinal allergic hypersensitivity reactions. This likely impacts the efficiency of interaction between the virus and mast cells, leading to less severe cytokine storm responses and symptoms. Therefore, fluvoxamine has the potential to reduce the cytokine storm pathway of severe SARS-CoV-2 infection.
Also, fluvoxamine inhibits the uptake of serotonin from platelets and therefore inhibits platelet aggregation. Fluvoxamine is a serotonin uptake inhibitor and inhibits serotonin concentration in platelets prior to clot formation. A 2011 study showed that patients taking SSRIs measured lower levels of coagulation than those that were not taking the drugs. Therefore, fluvoxamine has the potential to reduce the coagulation pathway of severe SARS-CoV-2 infection. Hyperinflammation following coagulation causes a number of health issues, including joint pain, gastrointestinal issues, and in some cases, brain injury. One player in inflammation is the sigma-1 receptor, which regulates endoplasmic reticulum mitochondrial calcium ion signalling, resulting in pro-inflammatory responses in higher concentrations. Fluvoxamine upregulates interleukin-10 (IL-10), which is an anti-inflammatory protein. The sigma-1 receptor downregulates other interleukins, such as IL-6 and IL-8, but not IL-10. Therefore high levels of IL-10 can inhibit the sigma-1 receptor and its hyperinflammatory processes. In other words, fluvoxamine may reduce COVID-related hyperinflammation. A rather elegant mechanism do you not agree?:
https://onlinelibrary.wiley.com/doi/full/10.1111/j.1440-18192011.02241.x
In other, unreported, news, we are at a turning point in global population history. Between 1950 and today, it was a widening of the entire pyramid – an increase of the number of children – that was responsible for the increase of the world population. From now on is not a widening of the base, but a ‘fill up’ of the population above the base: the number of children will barely increase and then start to decline, but the number of people of working age and old age will increase very substantially. As global health is improving and mortality is falling, the people alive today are expected to live longer than any generation before us. At a country level “peak child” is often followed by a time in which the country benefits from a “demographic dividend” when the proportion of the dependent young generation falls and the share of the population in working age increases. This is now happening at a global scale. For every child younger than 15 there were 1.8 people in working-age (15 to 64) in 1950; today there are 2.5; and by the end of the century there will be 3.4.
Richer countries have benefited from this transition in the last decades and are now facing the demographic problem of an increasingly larger share of retired people that are not contributing to the labour market. In the coming decades it will be the poorer countries that can benefit from this demographic dividend. The change from 1950 to today and the projections to 2100 show a world population that is becoming healthier. When the top of the pyramid becomes wider and looks less like a pyramid and instead becomes more box-shaped, the population lives through younger ages with very low risk of death and dies at an old age. The demographic structure of a healthy population at the final stage of the demographic transition is the box shape that we see for the entire world for 2100:
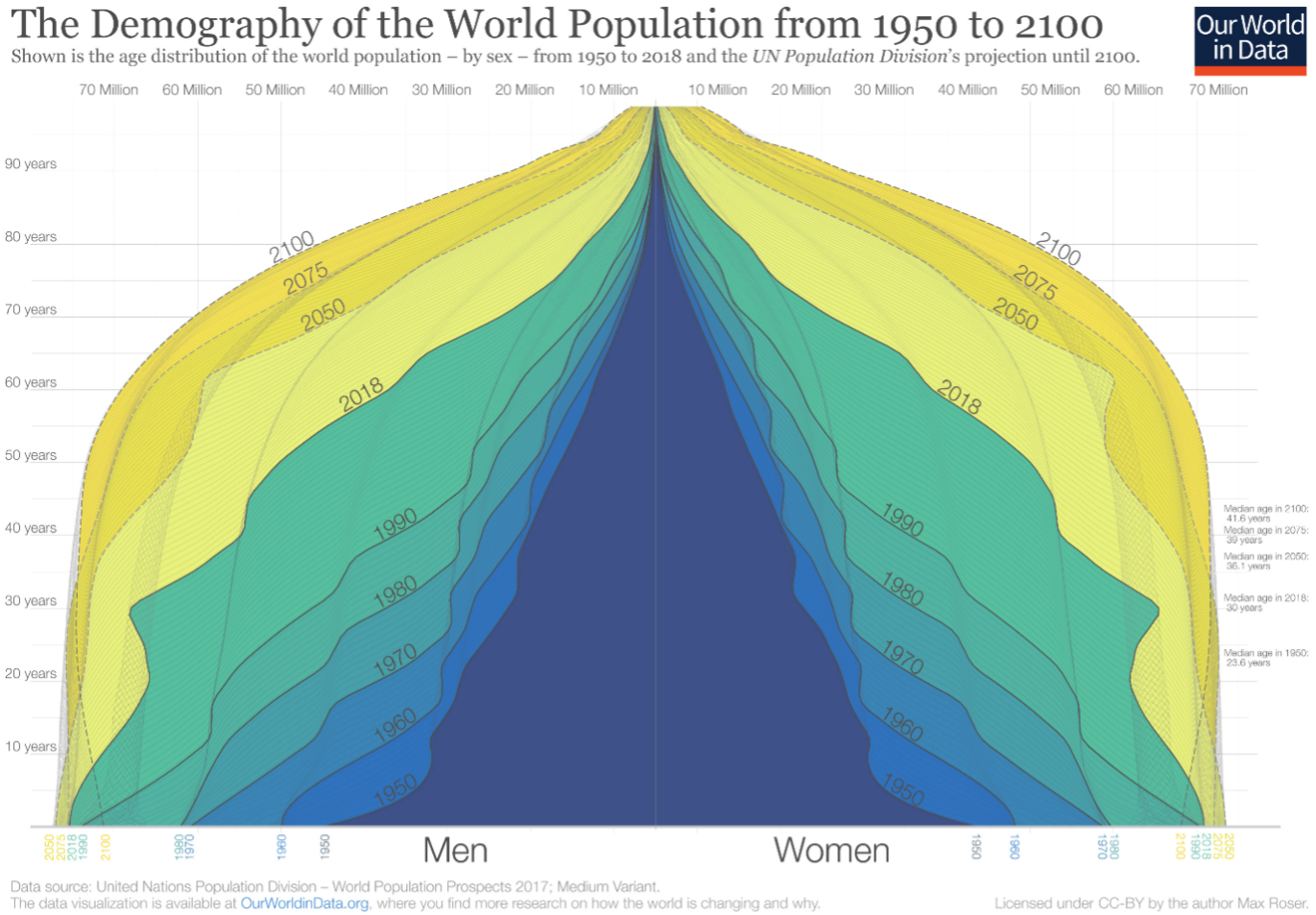
The timing varied significantly between countries – in higher income countries with low fertility rates and longer life expectancies, it has been shifting for decades. In the United States, under-5s were already outnumbered by those older than 64 by 1966. In Spain it was 1970; in South Korea it was 2000. For many countries, this crossover point is still to come. In India, it’s projected to be 2028. In South Africa, it’s expected to happen in 2036. In low-income countries with high fertility rates and lower life expectancy this point is still many decades away: it’s projected that in Nigeria, under-5s will outnumber those older than 64 until 2087. The number of children under 5 years old is projected to peak and plateau for most of the 21st century. And as the global population of people older than 64 years will continue to grow, it’s clear that we’re moving towards an ageing world and ageing worlds are less fit and more subject to epidemic, pandemic and routine outbreaks of disease:
https://ourworldindata.org/peak-child
Thanks for reading, keeping taking the right tablets and expanding the demographic pyramid.